Presenters: Dr. Lucía Miguel, Prof. Alfredo Adán
Case Summary:
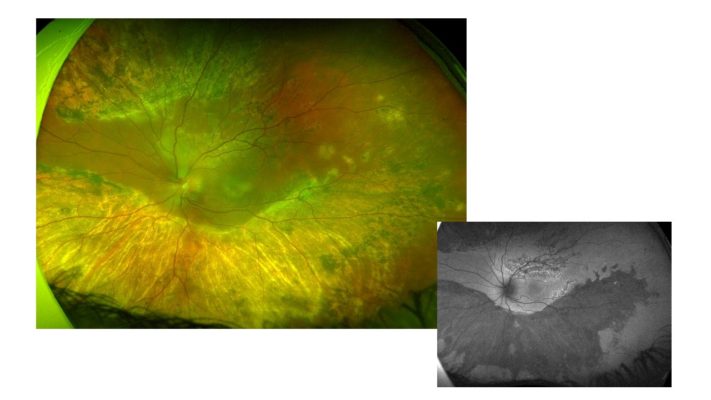
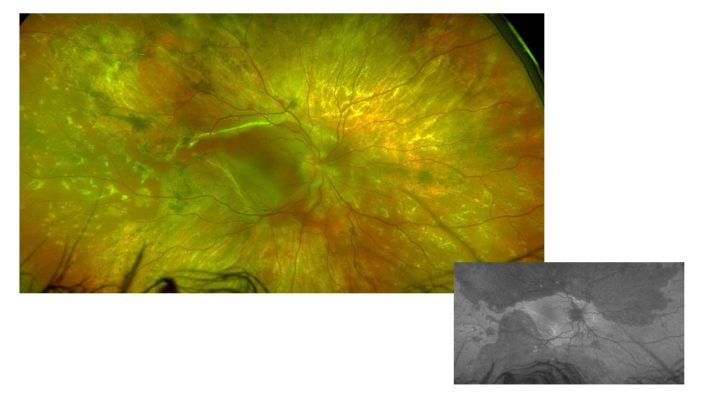
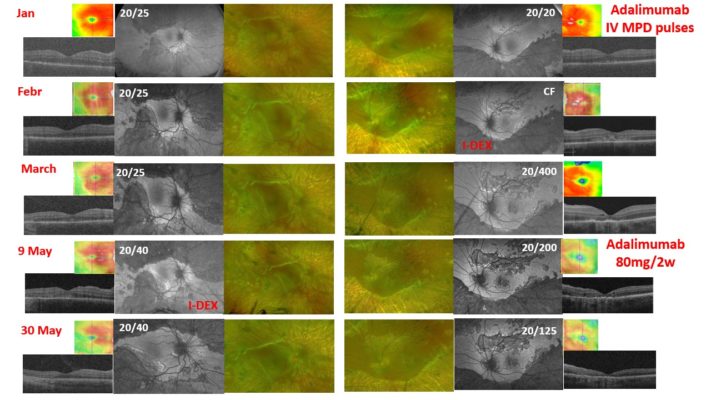
A 22-year-old man was referred for a stromal choroiditis of both eyes (OU). He had a medical history of a recent psychotic disorder. A first episode of non-granulomatous bilateral acute anterior uveitis occurred one month before. Visual acuity (VA) was 20/32 in OU. Funduscopy showed papillitis and vitreous haze 1+ in OS. Both eyes presented retinochoroidal lesions, some of them were pigmented, with a whitish demarcation line in the mid-periphery and the retinal arcades. OCT showed bilateral diffuse thickening. Fluorescein angiography showed bilateral hot disk. Some of the lesions showed early hypofluorescence and late hyperfluorescence, but not all. There was no vascular leakage. All ancillary tests, which included infections, autoimmunity, cranial MRI, among others, were negative. Prednisone 40mg daily was started. Visual acuity, vitritis, and papillitis improved, and the OCT normalized. Prednisone was decreased. Later, he was referred to our center. VA was 20/25 in OD, 20/20 in OS. In OS, the borders between the healthy retina and the scars showed a more active appearance and hyperautofluorescence was seen in the upper area. (Figure 1) Both optic nerves were greatly thickened. The OCT showed bilateral thickening with the external layers spared. Pulses of methylprednisolone were given and adalimumab was started. Less than a month later, VA in OS was counting fingers. He had received a total of three adalimumab injections and was on prednisone 7.5mg. He claimed to have good adherence to treatment. Whitish and creamy lesions had appeared at posterior pole in OS. They were hyperautofluorescent. OCT showed focal hyperreflective areas predominantly in outer layers. It was decided to treat with an intravitreal dexamethasone implant. Two weeks later, VA had improved to 20/400 and the lesions appeared more scarred and pigmented, and became hypoautofluorescent. Serum levels of adalimumab were 10.6 and anti-drug antibodies were negative. Two months later, VA of OD worsened (20/40). It presented a whitish band threatening the fovea. It was hyperautofluorescence. (Figure 2) OCT showed a subfoveal hyperreflective material. An intravitreal dexamethasone implant was decided. At the same time, the dose of adalimumab was intensified to 80mg every 2 weeks. Three weeks later, visual acuity remained at 20/40 in OD, although the patient reported a subjective improvement. The lesions appeared more inactive, with a scarred demarcation line. It also became hypoautofluorescent. At OCT the thickening had decreased and the hyperreflective material had disappeared, but there was a disruption in the outer layers. The nerve fiber layer in both eyes improved. An intravitreal fluocinolone implant has been injected into OD recently. We present this case of RELENTLESS PLACOID CHORIORETINITIS due to its frequent recurrences with threat of the fovea (Figure 3), to discuss the possibility of another alternative treatment.
Key Images:
Presented during EURETINA Case Club – Series 1, Episode 8 with Bahram Bodaghi and Carlos Pavesio (29 Jun, 2022) – RECORDING AVAILABLE TO MEMBERS ONLY.
Browse all cases from this Case Club




A mysterious bilateral stromal choroiditis in a young male patient – Alfredo Adan, Lucia Miguel





